Human Endocrine System
Endocrine system :
The endocrine system is also known as a chemical coordination system. The word endocrine derives from the Greek words "endo," meaning within; and "crinis," meaning to secrete. Higher animals have complex body organisation. Due to this, in addition to the nervous coordination system, there is a need for a chemical coordination system.

Chemical coordination is carried out by a collection of ductless glands (i.e. endocrine glands) of an organism, which controls body activities by means of chemical messengers called hormones. Here body activities includes; Metabolism, Chemical reactions, Water balance, Reproductive functioning, Body's growth, and Development, etc.
Major endocrine glands :
Hypothalamus :
The hypothalamus is ectodermal in origin. According to the typical division of the brain, it is the floor of the diencephalon of the forebrain. The floor of the hypothalamus continues as a downward projection called hypophyseal stalk or infundibulum which connects it to the hypophysis (pituitary gland) both physically and functionally by secretion of neurotransmitters.
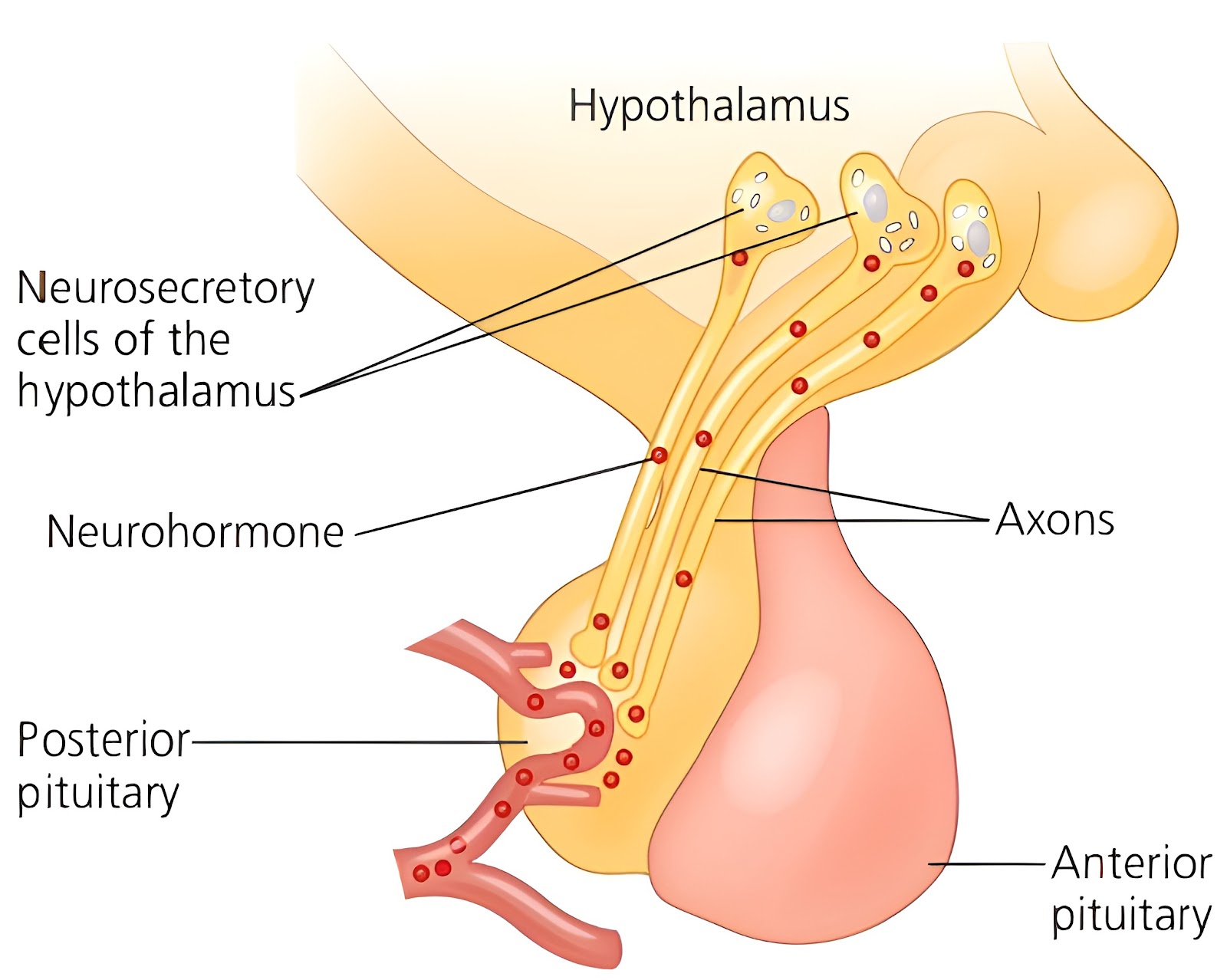
It is the area of the brain where nervous and endocrine systems are integrated, so it is a neuroendocrine structure. Therefore, it performs both; Nervous functions, as well as Endocrine functions. Major function of the hypothalamus is to maintain homeostasis. The hypothalamus controls stimulating and surprising activity of the pituitary gland by releasing and inhibiting hormones/neurohormones. They are secreted by the neurosecretory cells of the hypothalamus so they are called neurohormones. All hormones of hypothalamus are peptide hormones.
The pituitary gland controls almost all other endocrine glands, hence earlier it was called the master endocrine gland, but it is not proper to call it as master endocrine gland because it is itself under the control of the releasing hormones secreted by the hypothalamus of brain. Therefore, hypothalamus is known as the master switchboard or Supreme commander of endocrine regulation. The neurohormones of hypothalamus control the activity of the pituitary gland, but two hormones are synthesised in the hypothalamus by hypothalamic neurosecretory cells and are stored in the posterior pituitary lobe. These hormones are; ADH, and Oxytocin.
Pituitary gland :
The pituitary gland is also known as Hypophysis gland. The pituitary is an organ of dual origin. It is located just below the hypothalamus and is attached to it by a stalk called infundibulum or hypophyseal stalk. And roughly behind the bridge of your nose. Pituitary gland remains lodged in a bony depression called sella turcica of the sphenoid bone. The pituitary gland is the smallest endocrine gland, of diameter 1 to 1.5 cm. Pituitary gland is a pea sized reddish-grey coloured gland.
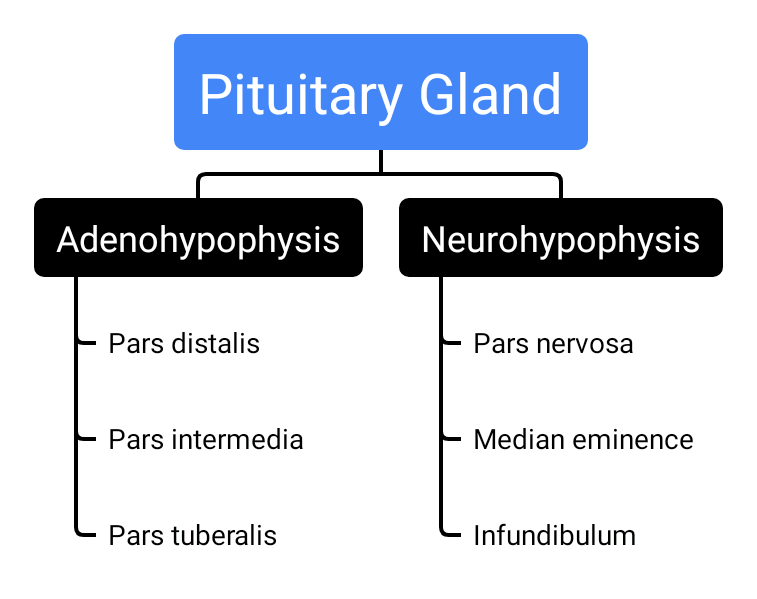
The pituitary gland is highly vascularized, like other endocrine glands. The pituitary gland controls almost all other endocrine glands, hence earlier it was called the master endocrine gland, but it is not proper to call it as master endocrine gland because it is itself under the control of the releasing hormones secreted by the hypothalamus of brain. Therefore, hypothalamus is known as the master switchboard or Supreme commander of endocrine regulation. The pituitary gland anatomically and functionally consists of two lobes, viz;
Anterior (front) pituitary lobe, and
Posterior (back) pituitary lobe.
Pars intermedia or Intermediate lobe is the boundary between the anterior and posterior lobes of the pituitary, and lying in the cleft between the anterior and posterior lob. Median eminence is defined as the more anterior portion of the posterior pituitary lobe that has a blood supply in common with the anterior pituitary lobe; specifically, the portal system. The median eminence is the functional link between the hypothalamus and the anterior pituitary gland. And it is composed of an extensive array of blood vessels and nerve endings.
Anterior pituitary lobe :
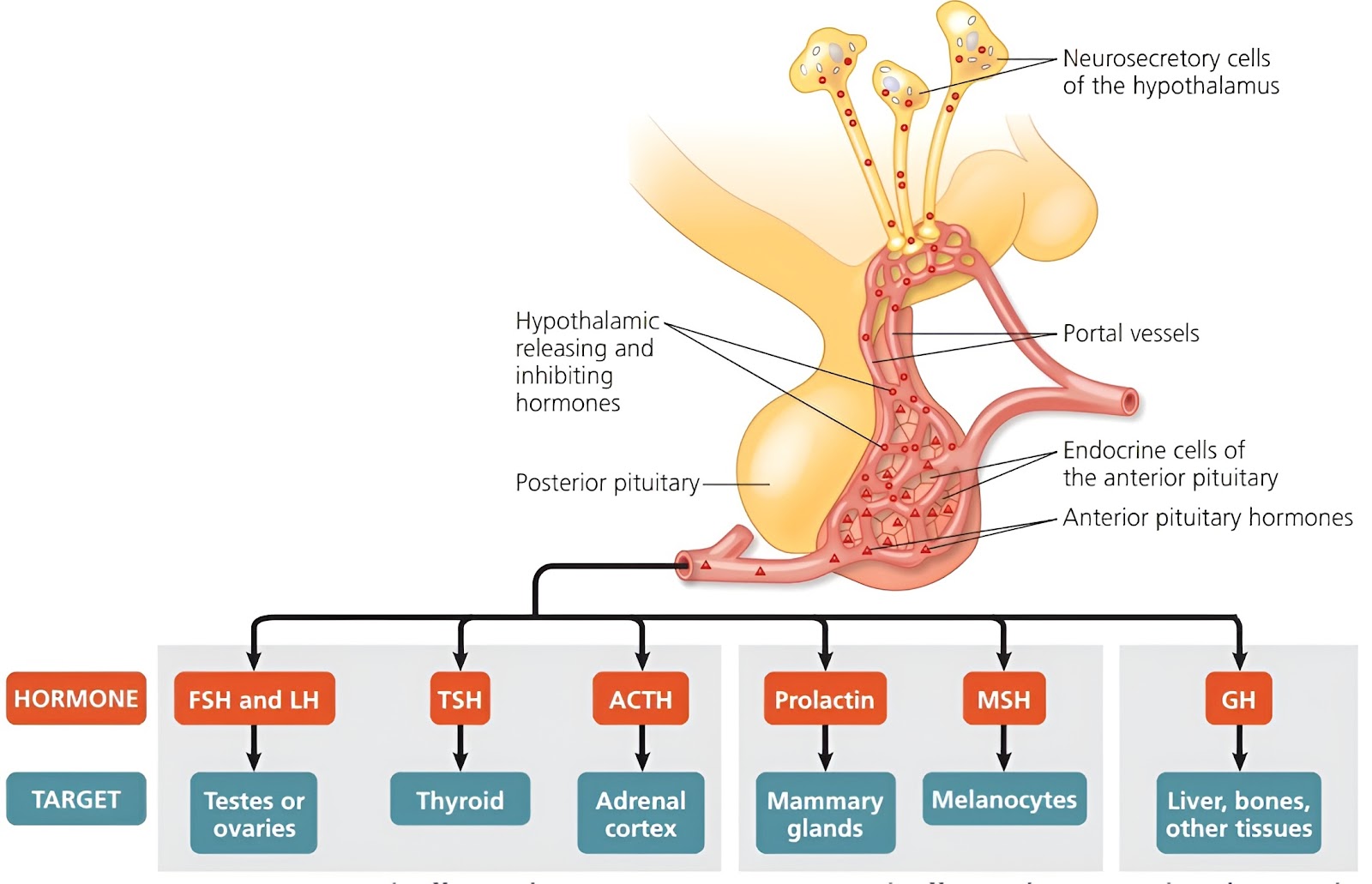
It is also called Adenohypophysis. Adenohypophysis comprises about 75% part of the pituitary gland. The anterior pituitary lobe (adenohypophysis) is derived from the oral ectoderm and is epithelial in origin. It consists of two parts, viz; Pars tuberalis (it forms a sheath around the infundibulum), and Pars distalis (it is the larger portion of pituitary gland). In the anterior lobe of the pituitary gland many hormones are synthesised, most of them are trophic hormones. Adenohypophysis and intermediate lobes are connected to the hypothalamus through the hypothalamic hypophyseal portal system.There are five types of cells found in an anterior pituitary lobe, this secrete seven different hormones. The cells and their hormones are;
Posterior pituitary lobe :
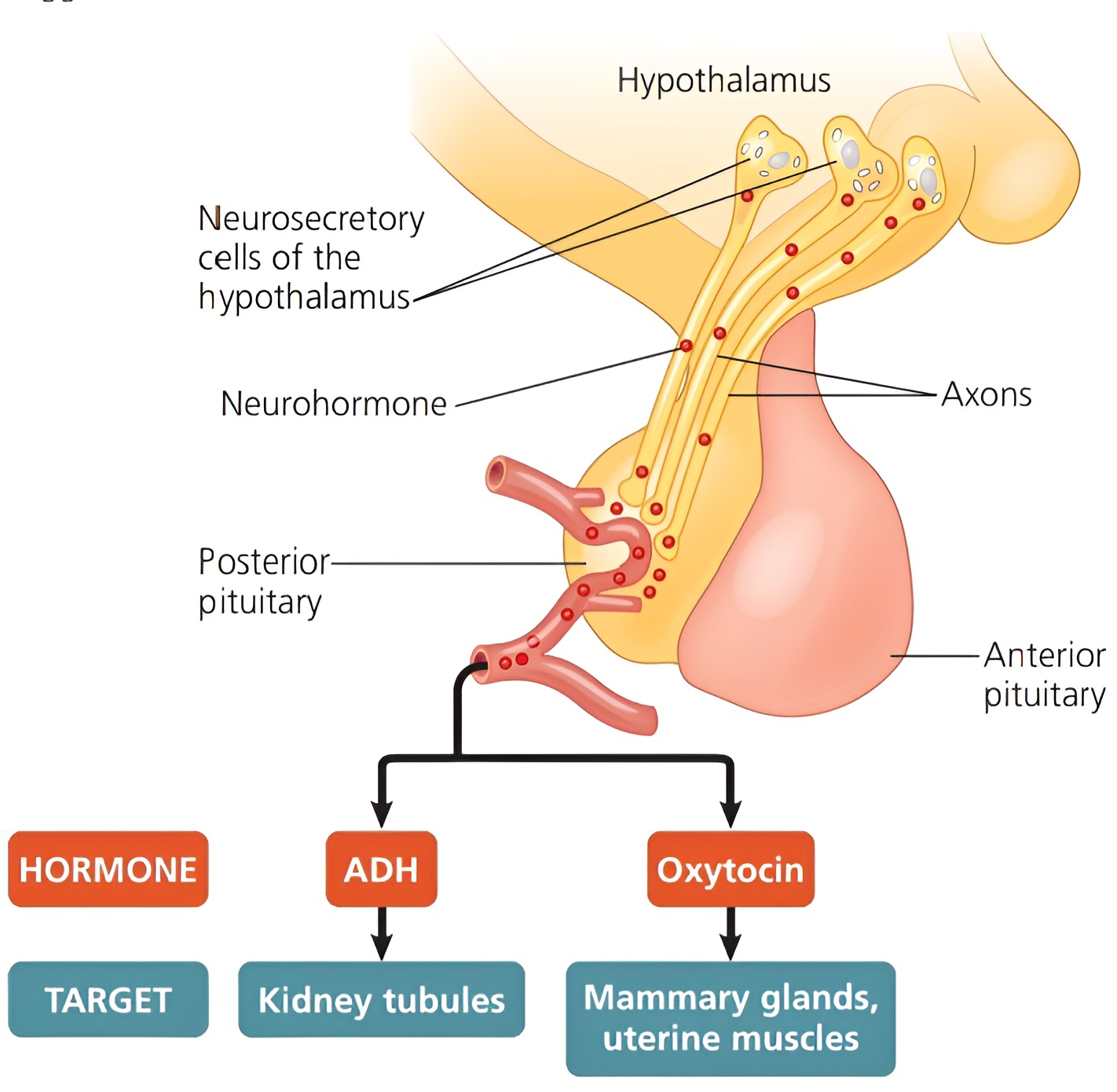
It is also called Neurohypophysis. Neurohypophysis comprises about 25% part of the pituitary gland. The posterior pituitary lobe (neurohypophysis) is derived from the neural ectoderm. It consists of two parts, viz, Pare nervosa (Neural lobe), and Infundibulum. In the posterior lobe of the pituitary gland no hormones are synthesised, but two hormones synthesised in the hypothalamus by hypothalamic neurosecretory cells and are stored in the posterior pituitary lobe. These hormones are; ADH, and Oxytocin. Neurohypophysis is connected directly to the hypothalamus by neurohypophysis portal system or axon fibres.
Pineal gland :
The pineal gland is also known as Pineal body or Pineal organ or Conarium or Epiphysis cerebri, and also called Third eye (historically) or Biological clock of the body because it shows rhythm in secretion of its hormones. It is ectodermal in origin. The pineal gland is reddish-grey in colour. Located between the cerebral hemispheres and roughly the centre of the brain, where it protrudes from the roof of the third ventricle of the brain or epi-thalamus. It is a small rounded body which consists of pineal cells and supporting glial cells. And the average mass of the panel varies from 0.1 to 0.2 g. It is highly vascularized, like other endocrine glands. It is a prominent gland till childhood but gradually it atrophies with onset of puberty.
It secretes two hormones, viz; Melatonin, and Serotonin. The pineal gland is sensitive to the biochemical signals of light. Therefore, the level of melatonin/ sleep hormone is more during scotophase ( or dark phase), while the level of serotonin is more during photophase (or light phase). Melatonin is derived from tryptophan and plays a very important role in the regulation of the Biological Clock (e.g. 24 hour diurnal rhythm) of our body. For example, it helps in maintaining the normal rhythms of; Sleep-wake cycle, Body temperature, Metabolism, Pigmentation, Reproductive cycles, as well as Our defence capability.
Thyroid gland :
The thyroid gland is endodermal in origin. It is reddish-brown in colour. Located in front of the trachea, anterior to the thyroid cartilage of the larynx (voice box) in the neck. It is a butterfly-shaped bilobed organ; Right thyroid lobe, and Left thyroid lobe. The two lobes are connected by a narrow central connective tissue called the isthmus, it is non-secretory. The microscopic structure of the thyroid gland shows thyroid follicles composed of cubical/ cuboidal epithelium resting on a basement membrane and filled with a homogenous material called gelatinous colloid. Small amount of loose connective tissue forms a stroma of the gland. The stroma contains blood capillaries and small groups of parafollicular cells or 'C' cells (clear cells). The thyroid gland is the largest endocrine gland.
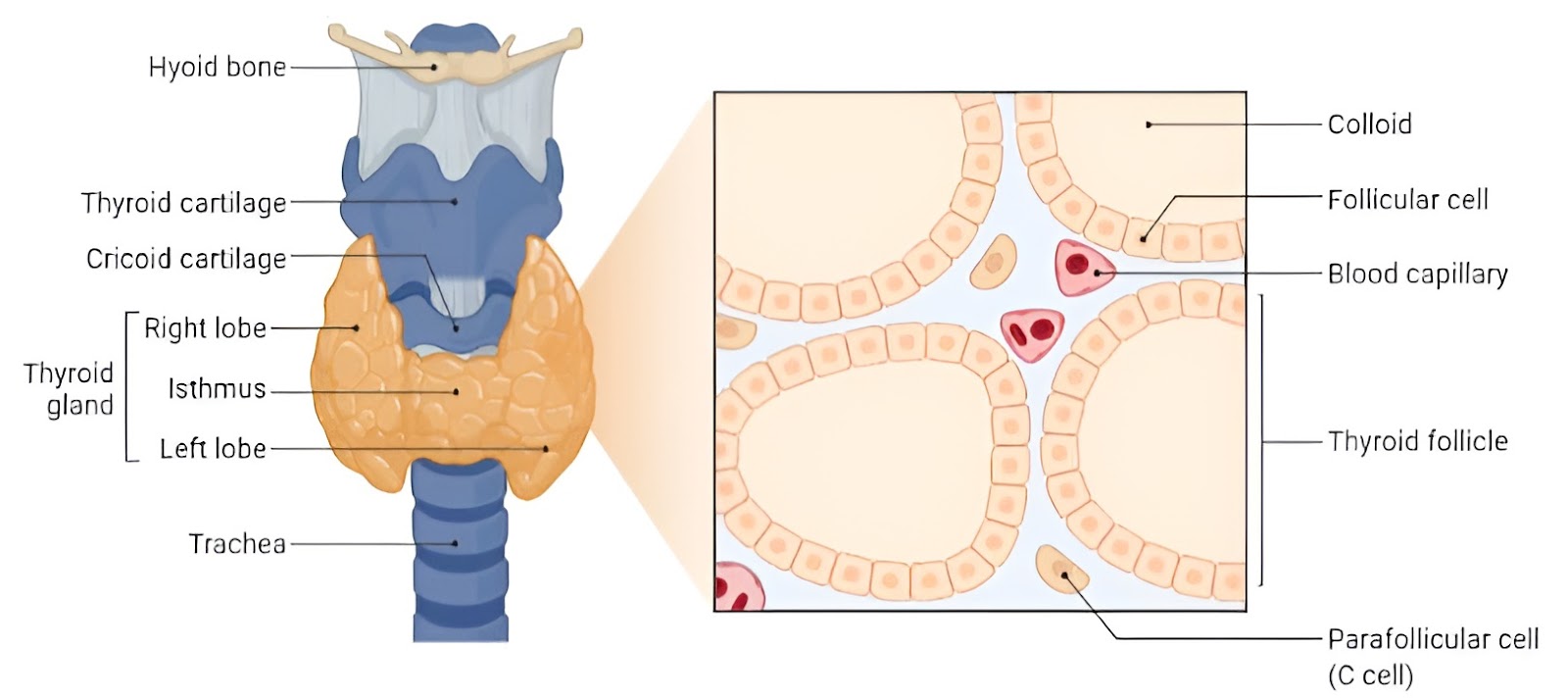
The thyroid gland requires iodine to sensitise its hormone. It is the only gland in the body which stores their production in large amounts for a long time (i.e. about 2 to 3 months and more). The thyroid gland is highly vascularized, like other endocrine glands. Thyroid gland is stimulated to secrete its hormones by thyroid stimulating hormone (TSH). The follicular cells of thyroid gland secrete a thyroid hormone (TH), which includes; T3 - Tri-iodothyronine/Thyroxine, and T4 - Tetra-iodothyronine. And parafollicular cells produce calcitonin hormone. Concentration of calcium and phosphate is maintained by parathormone and calcitonin. These two hormones form an antagonistic pair like insulin and glucagon.
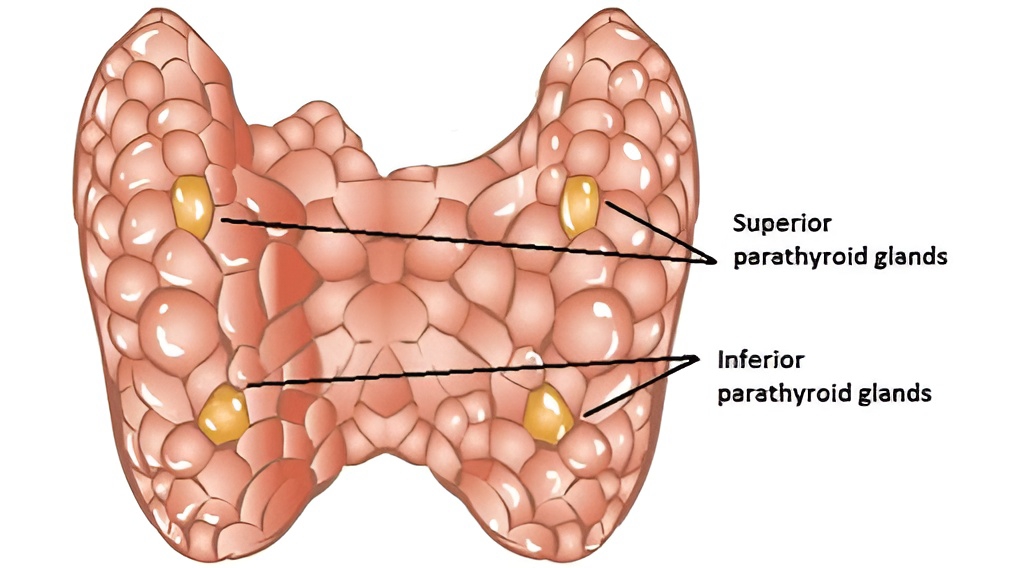
Parathyroid gland :
The parathyroid glands are endodermal in origin. The parathyroid gland is yellowish in colour. The parathyroid glands consist of four separate glands embedded in the posterior surface of the lobes of the thyroid gland. And they are named based on their position as; Superior parathyroid glands, and Inferior parathyroid glands. There are two types of cells present in the parathyroid gland, viz; Small chief cells (or principal cells), and Large oxyphil cells (or oxyntic or eosinophil cells). The chief cells are much more numerous than the oxyphil cells. The parathyroid gland is highly vascularized, like other endocrine glands.
The chief cells of the parathyroid secrete a hormone called parathyroid hormone (PTH) or parathormone and also called Collip's hormone. It doesn't need stimulation from any hormone from the pituitary and its secretion is dependent on a Ca+2 ion concentration. When the concentration decreases below the normal level, the parathyroid gland releases parathormone. It mobilises the release of calcium into the blood plasma and extracellular fluid, from the bones. Concentration of calcium and phosphate is maintained by parathormone and calcitonin. These two hormones form an antagonistic pair like insulin and glucagon.
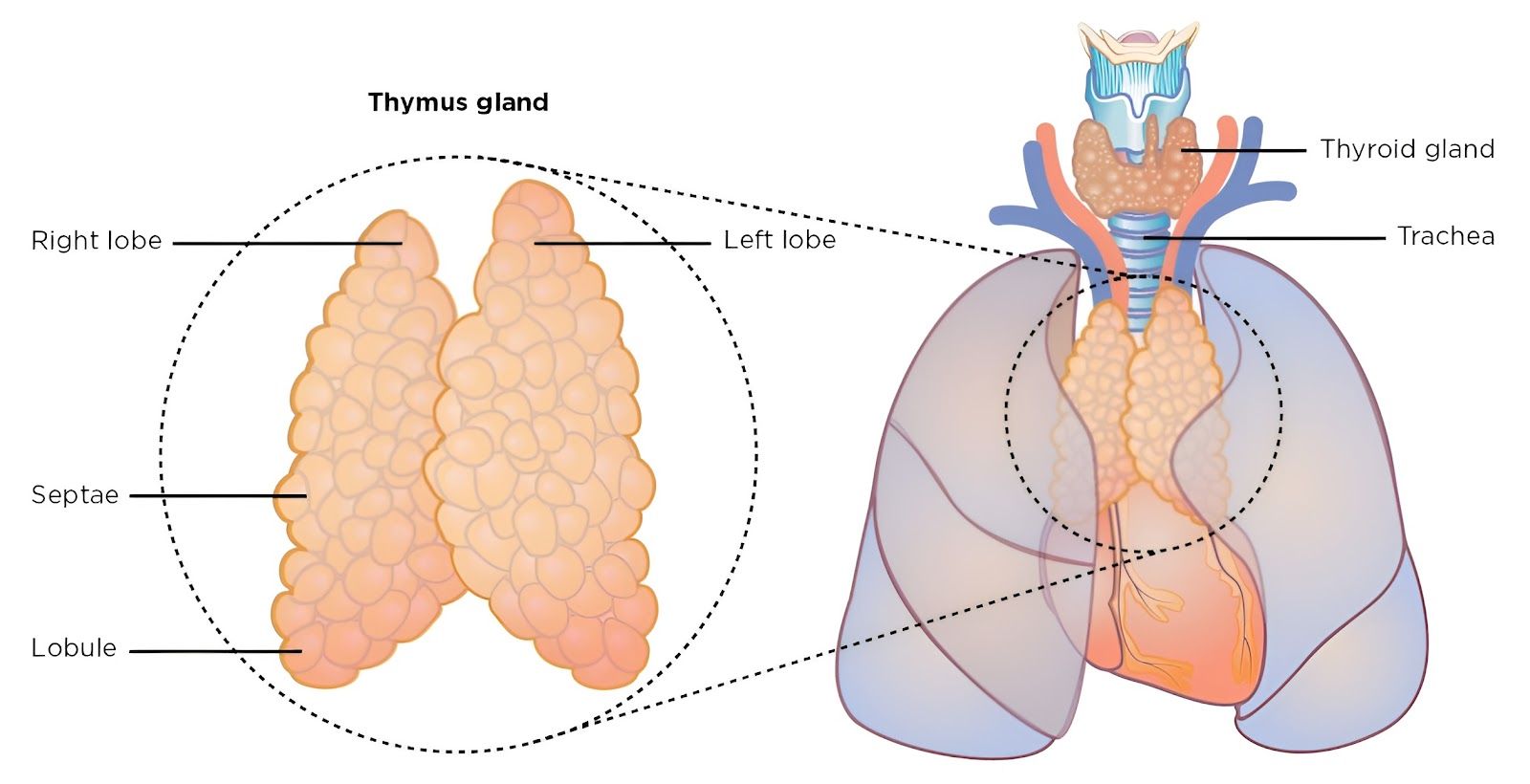
Thymus gland :
The thymus gland is also called the training school of T-lymphocytes or throne of immunity. This gland is bigger in size at birth. It grows in size until puberty, then the size gradually decreases, so it is called a temporary gland, and also Receding endocrine gland. According to the immunity theory of ageing, degeneration of the thymus is one the causes of ageing. The thymus gland is endodermal in origin. The thymus gland is soft in nature, and pinkish grey in colour. The thymus gland is present in the upper chest cavity on the trachea directly behind your sternum, on the dorsal side of the heart and between your lungs. It is a bilobed organ of lymphoid tissue, an enveloping layer of connective tissue holds the two lobes closely together, but a connective tissue capsule separates the two. Each thymic lobule consists of deeply-staining outer cortex, and lightly-staining central medulla. The thymus gland is highly vascularized, like other endocrine glands.
The thymus gland produces four different types of hormones, which are; Thymosin/thymine, Thymic humoral factor (THF), Thymic factor (TF), and Thymopoietin. Its functions are as follows; It controls the production of lymphocytes, Regulates transmission of minerals in bones, It plays some role in sexual development, and It also promotes production of antibodies by providing humoral immunity, etc.
Adrenal glands :
The adrenal glands in humans are suprarenal glands, and also emergency glands. The adrenal glands are the organ of dual origin. It is yellowish in colour. They are located on the upper border of each kidney. The adrenal glands are small, paird, conical shaped glands. A connective tissue capsule covers it. The adrenal gland is highly vascularized, like other endocrine glands. The adrenal glands show two distinct regions, viz; Adrenal Cortex, and Adrenal Medulla.
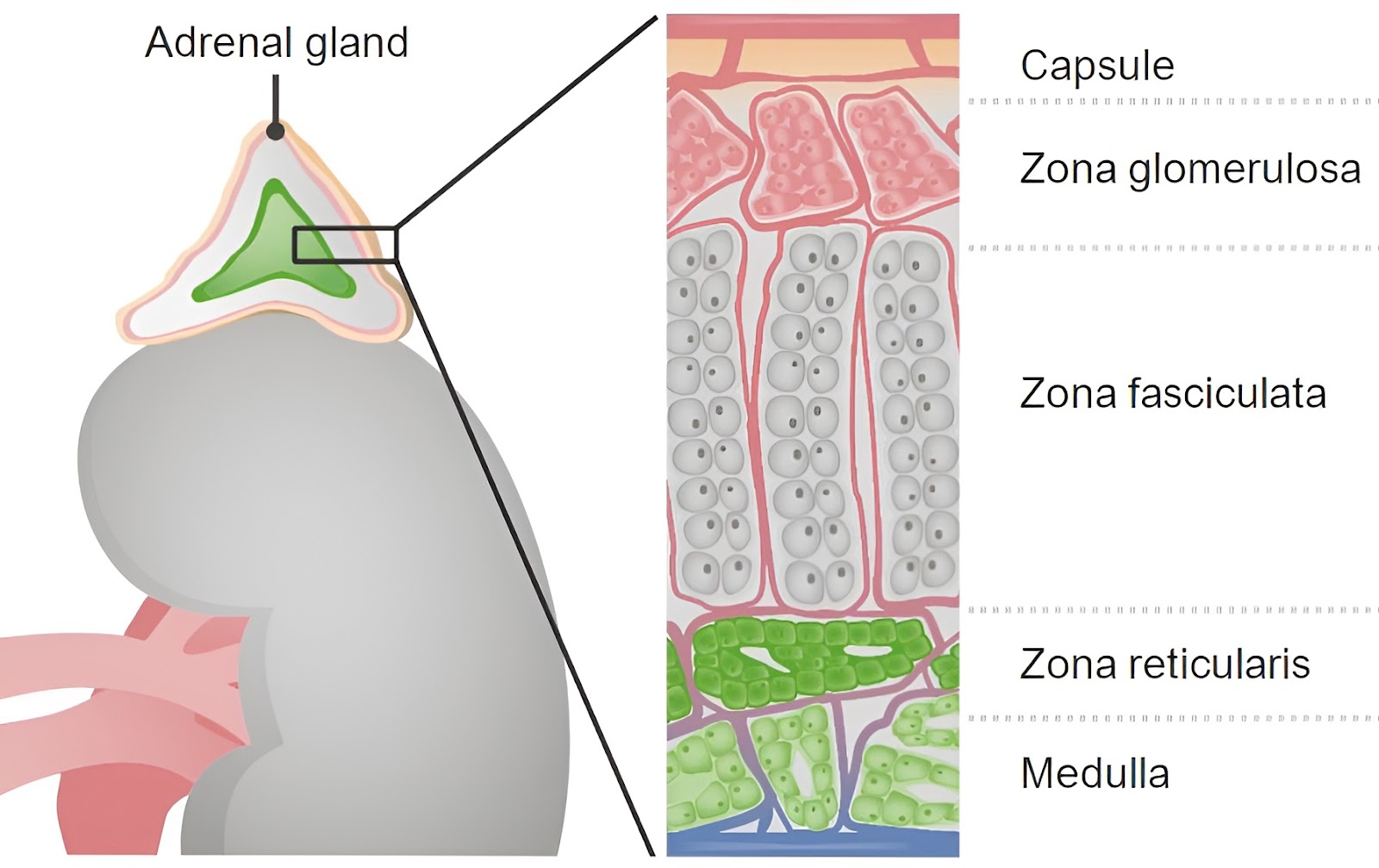
Adrenal Cortex :
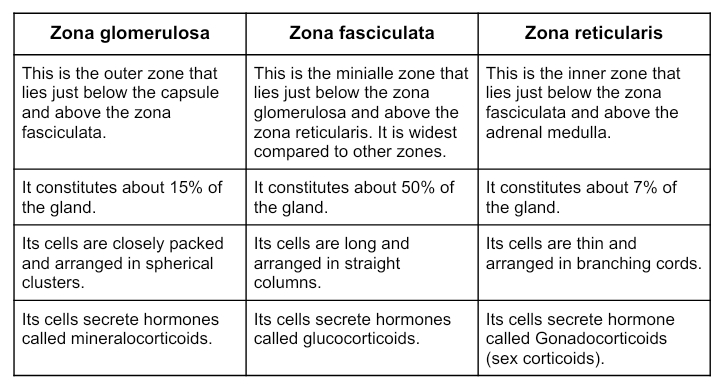
It is the outermost region of the gland. It constitutes about 80 to 90% of the gland. The adrenal cortex is derived from embryonic mesoderm. The adrenal cortex is essential for life. Adrenal cortex secretes many hormones that are together called corticoids. Corticoids are grouped into three categories, viz; Mineralocorticoids, Glucocorticoids, and Gonadocorticoids (sex corticoids). All hormones of the adrenal cortex are synthesised from cholesterol. The adrenal cortex is subdivided into three zones, viz; Zona glomerulosa, Zona fasciculata, and Zona reticularis.
The cells of the zona fasciculata and zona reticulata contain ascorbic acid (vitamin C).
Adrenal Medulla :
It is the innermost region of the gland. It constitutes about 10 to 20% of the gland. The adrenal medulla is derived from embryonic ectoderm. The adrenal medulla consists of rounded groups of relatively large and granular cells, these are called chromaffin cells and also neuro-endocrine cells. These cells are connected with the preganglionic motor fibres of the sympathetic nervous system. These cells of adrenal medulla synthesise two hormones from amino acid Tyrosine, which are; Norepinephrine (also called Noradrenaline), and Epinephrine (also called Adrenaline). Norepinephrine and epinephrine are derived from Tyrosine amino acids.

Pancreas :
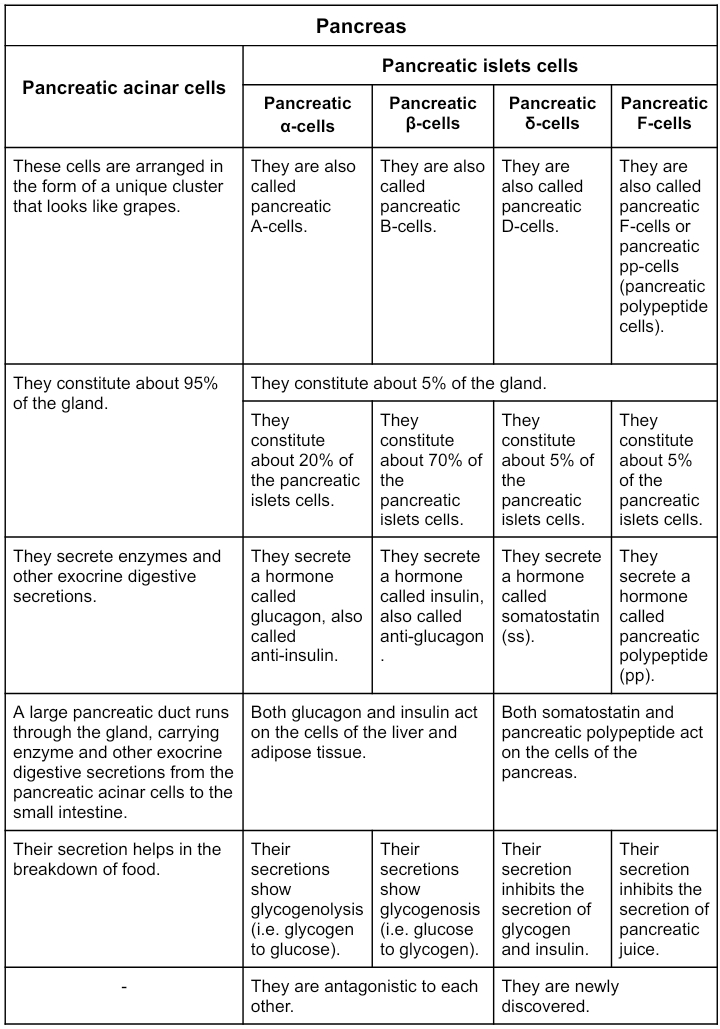
The pancreas is endodermal in origin. It is reddish-grey in colour. Located posterior/ behind to stomach. And also it is surrounded by other organs including: Small intestine, Liver and Spleen. It is a leaf shaped gland or V-shaped organ. The body and tail extends laterally, with its head in the curve of duodenum and tail touches the spleen. The pancreas is a both exocrine as well as endocrine gland, therefore; it is heterocrine or dual gland.

The tissue of the pancreas has two types of cluster of cells, which are; Pancreatic acini or pancreatic lobules, and Pancreatic islets or islets of langerhans. Four kinds of cells have been identified in the pancreatic islets, which are; Pancreatic α-cells or Pancreatic A-cells, Pancreatic β-cells or Pancreatic B-cells, Pancreatic δ-cells or Pancreatic D-cells, and Pancreatic γ-cells or Pancreatic F-cells or Pancreatic pp-cells (Pancreatic polypeptide cells).
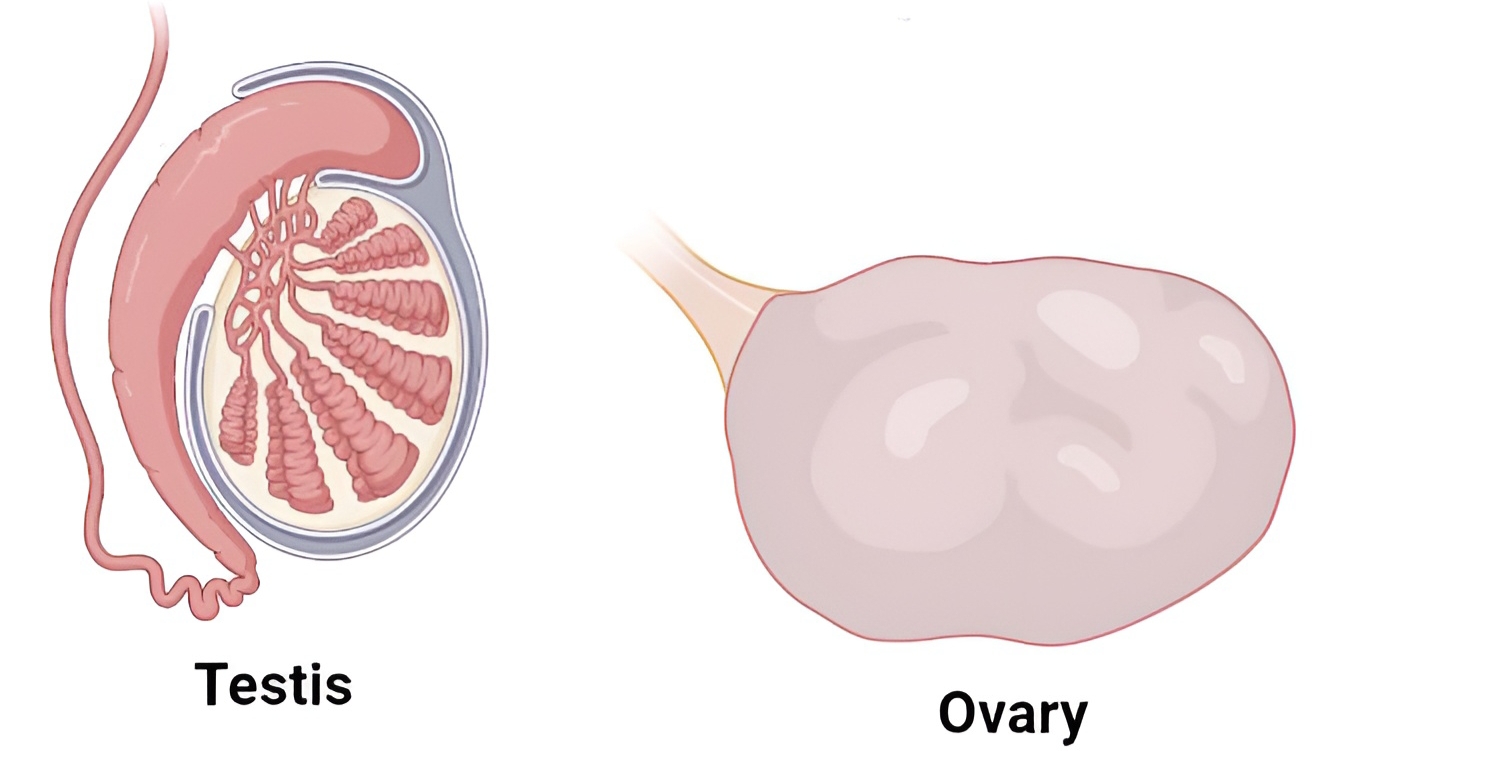
Gonads :
Gonads are the male and female primary reproductive organs. The male gonads are the testes and the female gonads are the ovaries. The testes has two functions, viz; Spermatogenesis, and Hormone production. Similarly, the ovaries have two functions, viz; Oogenesis, and Hormone production. The testicular and ovarian hormones are categorised into two types; Steroid hormones, and Proteinaceous hormones. Steroidal hormones of gonads include; Androgens (Testosterone), Progestin and Oestrogen. Proteinaceous hormones of gonads include; Inhibin and Relaxin.
Major composed endocrine glands :
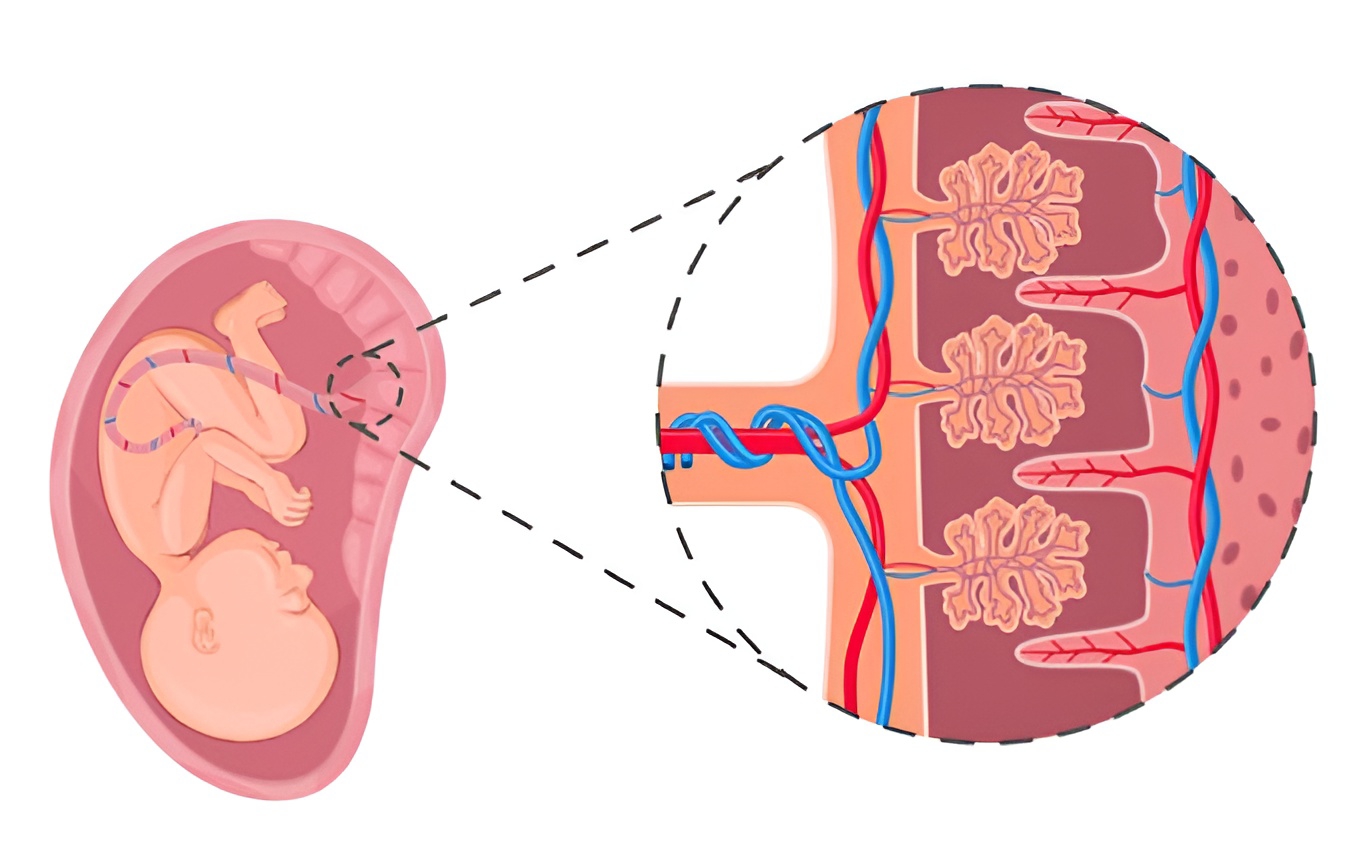
Placenta :
The maternal surface of the placenta should be dark maroon in colour. During pregnancy, placenta secretes hormones, such as; Oestrogen, Progesterone, Human chorionic gonadotropin (hCG), and Human placental progesterone. These hormones check the contraction of uterine muscles and also maintain the thickness of uterine endometrium thus they help to maintain pregnancy.
Gastro-intestinal tract :
In the gastrointestinal mucosa, certain cells are endocrine in function. These cells produce hormones which play vital roles in digestive processes and flow of digestive juices.
Gastrin : It stimulates gastric glands to produce gastric juice.
Secretin : It is responsible for secretion of pancreatic juice and bile from presence and liver.
Cholecystokinin (CCK) or Pancreozymin (PZ) : This hormone stimulates the pancreas to release its enzymes and also stimulates gallbladder to release bill.
Entero-gastrone or Gastric inhibitory peptide (GIP) : It slows gastric contractions and inhibits the secretion of gastric juice.

Kidney :
It produces; Renin, Erythropoietin, and Calcitriol (it is the active form of vitamin cholecalciferol (D3)).
Heart :
It produces Atrial natriuretic hormone (ANF), increases sodium excretion by kidneys and reduces blood pressure.
Major hormones in endocrine system :
Growth hormone (GH) :
This hormone is also known as Somatotropin hormone (STH) or Human growth hormone (hGH). It is a peptide (small sequence of amino acids) hormone. This hormone is secreted by the cells from the anterior pituitary lobe called Somatotrophs. The secretion of this hormone from anterior pituitary lobe of pituitary gland is stimulated by growth hormone-releasing hormone (GHRH), while inhabited by growth hormone-inhibiting hormone (GHIH) or Somatostatin aslo it inhabit the secretion of thyroid stimulating hormone, this two regulating hormones are secreted from hypothalamus. In addition, somatostatin is produced in the pancreas and inhibits the secretion of other pancreatic hormones such as insulin and glucagon.
The target tissues/cells of growth hormone are various body cells which undergo growth. The principal action of this hormone is to stimulate growth and development of all tissues by accelerating protein synthesis and cell division. This hormone also acts on the liver cells, in response the liver produces Somatomedins (insulin-like growth factor). Highest secretion of the GH is seen till puberty and then its secretion becomes low. However, it is continuously secreted throughout life for repair and replacement of body tissue or cells.
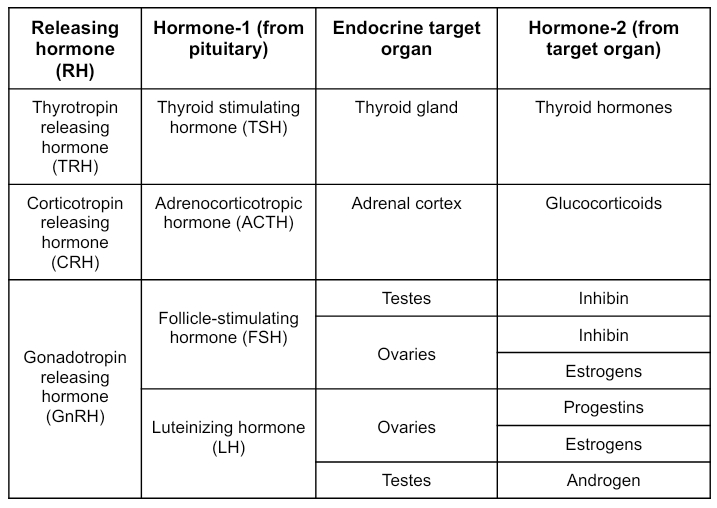
Thyroid stimulating hormone (TSH) :
This hormone is also known as Thyrotropin. It is a peptide hormone. This hormone is secreted by the cells from the anterior pituitary lobe called Thyrotrophs. The secretion of this hormone from anterior pituitary lobe of pituitary gland is stimulated by thyrotropin-releasing hormone (TRH), while inhabited by thyroxine (i.e. T4 and T3) from thyroid gland, and also by Somatostatin; also it inhibits the secretion of growth hormone, these two regulating hormones are secreted from hypothalamus.
The target tissues/cells of thyroid stimulating hormone are cells of the thyroid gland. The principal action of this hormone is to stimulates secretion of thyroid hormones or Thyroxine (i.e. T4 and T3). Here; T3 is Tri-iodothyronine, and T4 is Tetra-iodothyronine.
Gonadotropic hormones :
This hormone is also known as Gonadotropins. It is peptide glycoprotein, a polypeptide hormone. This hormone is secreted by the cells from the anterior pituitary lobe called Gonadotrope. The secretion of this hormone from anterior pituitary lobe of pituitary gland is stimulated by Gonadotropin-releasing hormone (GnRH), while inhabited by Gonadotropin-inhibitory hormones (GnIH), this two regulating hormones are secreted from hypothalamus. The target tissues/cells of gonadotropins are cells of gonads (i.e. testes in males and ovaries in females). The principal action of this hormones are;
Luteinizing hormone (LH) :
In females, the luteinizing hormone helps in ovulation (discharge of ovum from graafian follicle). And also it stimulates the corpus luteum of the ovary to secrete progesterone In male it activates the Leydig's (interstitial) cells of the test is to secrete androgens hence it may be called interstitial cell stimulating hormone (ICSH) in male.
Follicle stimulating hormone (FSH) :
In females it acts on ovaries and stimulates growth of ovarian follicles and their secretion of oestrogens, while in male it acts on sertoli cells and stimulates spermatogenesis (formation of sperms) and development of seminiferous tubules.
Prolactin (PRL) :
This hormone is also known as Mammotropin hormone (MTH) or Hormone of maternity, because its main physiological effect is to activate growth of breasts during pregnancy and secretion of mammary glands after child birth. Or Luteotropic hormone (LTH), because it also stimulates the corpus luteum of the ovary to secrete progesterone hormone. It is a peptide hormone. This hormone is secreted by the cells from the anterior pituitary lobe called Lactotrophs. The secretion of this hormone from the anterior pituitary lobe of the pituitary gland is stimulated by Stimulation of the nipples and mammary gland, as occurs during nursing leading to prolactin release. This effect appears to be due to a spinal reflex arc that causes release of prolactin-stimulating hormones (PSH) or prolactin-stimulating factor(PSF) from the hypothalamus.
The target tissues/cells of prolactin are cells of mammary glands and other sex accessory organs. The principal action of this hormone is to promote milk production (lactation).
Adrenocorticotropic hormone (ACTH) :
This hormone is also known as Adreno-corticotropin or Corticotropin. It is a peptide hormone. This hormone is secreted by the cells from the anterior pituitary lobe called Corticotrophs. The secretion of this hormone from the anterior pituitary lobe of the pituitary gland is stimulated by Corticotropin-releasing hormone(CRH) from hypothalamus, while inhabited by glucocorticoids from adrenal cortex.
The target tissues/cells of this hormone are cortex regions of adrenal glands (i.e. adrenal cortex). The principal action of this hormone is to stimulate the secretion of glucocorticoids.
Melanocyte Stimulating Hormone (MSH) :
This hormone is also known as Melanotropin. It is a group of specialised peptide hormones. The secretion of melanotropin from anterior pituitary lobe and pars intermedia of pituitary gland and also from skin is stimulated by ultraviolet light (uv), where it increases synthesis of melanin. And it is also produced from the hypothalamus of the diencephalon region of the brain.
The target tissues/cells of melanotropin are melanocytes in skin. This hormone is important for protecting the skin from UV rays, development of pigmentation (it is the major reason for darkness of skin) and control of appetite.
Antidiuretic hormone(ADH) :
This hormone is also known as Vasopressin or Pitressin. In the posterior lobe of the pituitary gland no hormones are synthesised, but this hormone, synthesised in the hypothalamus by hypothalamic neurosecretory cells, remains stored in it. Neurohypophysis is connected directly to the hypothalamus by neurohypophyseal portal tract or axon fibres. The target tissues/cells of this hormone are cells of kidneys. This hormone has two functions;
Antidiuretic effect : It increases the reabsorption of water in the distal convoluted tubule (DCT) and collecting ducts of the nephrons of the kidneys. As a result, the reabsorption of water from the glomerular filtrate is increased. And decreases loss of water by reducing the urine quantity. Simply the concentration of our urine is controlled by this hormone.
Pressor effect : Involuntary muscles in the walls of the intestine, gallbladder, urinary bladder and blood vessels are stimulated to contract by ADH. Contraction of the walls of the blood vessels raises the blood pressure and this may be its most important pressure effect.
Oxytocin (OT) :
This hormone is also known as Birth hormone or Milk ejecting hormone or Love hormone. In the posterior lobe of the pituitary gland no hormones are synthesised, but this hormone, synthesised in the hypothalamus by hypothalamic neurosecretory cells, remains stored in it. Neurohypophysis is connected directly to the hypothalamus by axon fibres.
The target tissues/cells of this hormone are Cells of mammary glands. The principal action of this hormone is to stimulate contraction of the uterus during parturition. It also stimulates the contraction of mammary glands to initiate ejection or release of milk.
Mineralocorticoids :
These hormones are secreted by the cells of the zona glomerulosa of the adrenal cortex. As the name indicates, they are responsible for the regulation of mineral metabolism.
Aldosterone (salt-retaining hormone) is the principal mineralocorticoid (90 to 95%) in humans. Like all other hormones of the adrenal cortex, aldosterone is a steroid hormone. Its main function is to regulate the sodium content of the body. It is secreted when the sodium level is low. It acts on the cells of kidneys to cause more sodium to be returned to the blood and more potassium to be excreted. As the sodium concentration in the blood increases, water follows it by osmosis, so the blood volume also increases. Thus the effect of aldosterone is to increase both sodium and water in the blood.
Glucocorticoids :
These hormones are secreted by the cells of the zona fasciculata of the adrenal cortex. As the name indicates, they are responsible for the carbohydrate metabolism, however, they also affect the metabolism of proteins and fats. Glucocorticoids include three main hormones; Cortisol (Hydrocortisone), Corticosterone, and Cortisone.
Of the three, cortisol is the most abundant (about 95%). It stimulates the liver cells to synthesise carbohydrates from non-carbohydrates such as; amino acids and glycerol, thus increasing the level of glucose in the blood. Cortisol also stimulates the degradation of proteins within cells and amino acids in the blood, therefore, increases the level of amino acids in the blood. A third effect of cortisol is to stimulate the break-down of fats in adipose tissue and release fatty acids into the blood. Thus cortisol has an anti-insulin effect. It also helps in reducing pain. Cortisol is anti-inflammatory. Cortisol is also "immunosuppressive", it suppresses synthesis of antibodies by inhibiting the production of lymphocytes in the lymphoid tissues. That is why cortisol is used for treatment of allergies. It is also used in transplantation surgery to suppress the formation of antibodies in the body of recipients so that the latter may accept the transplanted organs. This hormone increases RBC count, but decreases the WBC count of blood. It also elevates blood pressure. Cortisol has the capacity to cope with stress, when we are under stress our body secretes cortisol that is why this hormone is called "stress hormone".
Gonadocorticoids :
These hormones are secreted by the cells of the zona reticularis of the adrenal cortex. They are also called sex hormones of adrenal glands. Large quantities of male than female sex-corticoids (sex hormones) are produced. These male sex hormones are called androgens which are important in the development of a male foetus. Although the genetic sex is determined by the chromosomes in a fertilized egg, a male foetus develops normal male characteristics only if the foetal gonads and adrenal glands produce sufficient quantities of androgens. Therefore, androgens stimulate the development of male secondary sexual characters like distribution of body hair. Female sex hormones secreted by the adrenal cortex are oestrogens which maintain the development of female secondary sexual characters.
Norepinephrine (Noradrenaline) :
These hormones are secreted by the cells of adrenal medulla. It regulates blood pressure under normal conditions. It causes constriction of essentially all the blood vessels of the body. It causes increased activity of the heart, inhibition of gastrointestinal tract, dilation of the pupils of the eyes and so forth.
Epinephrine (Adrenaline) :
These hormones are secreted by the cells of adrenal medulla. It is secreted at the time of emergency. Hence it is also called emergency hormone and also 3F Hormone - (fright, fight, flight).
Testosterone :
It is secreted from interstitial cells or leydig cells by the influence of luteinising hormone (LH). Rise in testosterone level in blood above normal inhibits LH secretion. It is also responsible for appearance of secondary sexual characters such as; Facial and pubic hair, Deepening of voice, Broadening of shoulders, and Male aggressiveness, etc. It also helps in maintenance of testes.
Progesterone :
It is secreted by the corpus luteum of the ovary after ovulation. This hormone is essential for thickening of uterine endometrium, thus preparing the uterus for implantation of fertilised ovum. It is responsible for development of mammary glands during pregnancy. It inhibits uterine contractions during pregnancy.
Oestrogen :
These are secreted by developing follicles. Estradiol is the main oestrogen. It is responsible for secondary sexual characters in female.
Inhibin :
It is secreted by the corpus luteum. Inhibin inhibits the FSH and GnRH production.
Relaxin :
It is secreted by the corpus luteum of the ovary at the end of gestation period. It relaxes the cervix of the pregnant female and ligaments of pelvic girdle for easy birth of young one.
Tropic hormones :
Tropic hormones are hormones that have other endocrine glands as their target. They are also known as Tropins. Most tropic hormones are produced and secreted by the anterior pituitary.
Hypothalamic-hypophyseal portal system :
Portal System is a vascular arrangement in which blood from the capillaries of one organ is transported to the capillaries of another organ by a connecting vein or veins. Adenohypophysis and intermediate lobes are connected to the hypothalamus through the hypothalamic-hypophyseal portal system. The hypothalamic-hypophyseal portal system allows the transportation of thalamic hormones to the anterior pituitary lobe along with blood.

Disorders of endocrine system :
Disorders of the endocrine system often involve either; hyposecretion or hypersecretion of a particular hormone. In other cases, the problem is faulty hormone receptors or inadequate number of receptors. And also defects in second messenger systems.
Disorders related to pituitary gland :
Pituitary disorders are most commonly caused by a pituitary adenoma, a benign (non-cancerous) pituitary tumour. Due to pituitary adenoma, pituitary gland makes too much or too little of a particular hormone, based on this pituitary disorders are classified as; Hyperpituitarism, and Hypopituitarism.
Hyperpituitarism :
In this case pituitary adenoma are non-functioning, meaning that they do not produce any hormone themselves, but cause an inadequate production of one or more pituitary hormones due to the physical pressure of the growing tumour on the glandular tissue. In this case simply the pituitary gland produced large enough hormones due to hyperactivity of the pituitary gland.
Hypersecretion of Growth hormone :
Gigantism :
In childhood, hypersecretion (excess secretion) of GH leads to gigantism. It is a condition of overgrowth wherein an individual attains abnormal height. The person grows to be very tall, but body proportions are about normal.

Sultan Kösen,
Turkish farmer
Acromegaly :
In middle aged adults, hypersecretion (excess secretion) of GH leads to acromegaly. It is a condition of abnormal elongation of long bones of arms, legs, fingers, feet, and also lower jaw. Eyelids, lips, tongue, and nose enlarge, skin thickens and develops furrows, especially on the forehead and soles.

The Great Khali,
Indian professional wrestler
Hypopituitarism :
In this case pituitary adenoma are non-functioning, meaning that they do not produce any hormone themselves, but pituitary gland fails to produce one or more hormones, or doesn't produce enough hormones due to the physical pressure of the growing tumour on the glandular tissue. In this case simply the pituitary gland is not sufficient to produce enough hormones due to hyperactivity of the pituitary gland.
Hyposecretion of Growth hormone :
Dwarfism :
In childhood, hyposecretion (insufficient secretion or deficiency) of GH leads to dwarfism. It is a condition of retardation of physical growth. Other organs of the body also fail to grow, and the body proportions are childlike.

Jyoti Amge,
Indian actress
Hyposecretion of ADH :
Diabetes insipidus (DI) :
The most common abnormality associated with dysfunction of the posterior pituitary is diabetes insipidus (the word diabetes means metabolic disorder; and Insipidus means testless, absence of glucose in urine). This disease is commonly known as Drinkers disease. Based on the position dysfunction, there are two types of DI;
Neurogenic DI :
It results from hyposecretion of ADH, usually caused by a brain tumour, head trauma, or brain surgery that damages the posterior pituitary or the hypothalamus. Treatment of neurogenic diabetes insipidus involves hormone replacement, usually for life.
Nephrogenic DI :
In this, kidneys do not respond to ADH. Treatment of nephrogenic diabetes insipidus is more complex and depends on the nature of the kidney dysfunction. Because so much water is lost in the urine (diuresis), a person with DI may die of dehydration if deprived of water for only a day or so.
Sign and symptoms of DI :
Excess urine output (i.e. polyuria) No glucose is lost in the urine, due to reduced water reabsorption by nephrons of the kidney,
Excessive micturition causes dehydration and excess thirst (i.e. polydipsia).
Fatigue,
Headache,
Dehydration,
Flushing of face,
Water-electrolyte imbalance,
Insomnia,
Irritability,
Muscle weakness,
Weight loss,
Confusion or non-responsiveness,
Tremor,
Dizziness,
Anxiety or nervousness,
Shortness of breath,
High blood pressure (i.e. fast heart rate), etc.
Treatment :
Depending on the form of the disorder, treatments might include hormone therapy, a low-salt diet and drinking more water.
Disorders related to thyroid gland :
Hypersecretion of thyroid hormone (Hyperthyroidism) :
It is caused by an increase in the levels of thyroid hormones, due to a tumour of thyroid glands.
Graves disease :
In adulthood, hypersecretion (excess secretion) of TH (or hyperthyroidism) leads to Graves disease. The graves disease is also called exophthalmic goitre. It is an autoimmune disorder in which the person produces antibodies that mimic the action of thyroid-stimulating hormone (TSH). The antibodies continually stimulate the thyroid gland to grow and produce thyroid hormones.

Sign and symptoms of graves disease :
Excess sweating,
Fatigue,
Diarrhoea,
Goitre (ie. enlarged thyroid gland),
Hair loss,
Hand tremor,
Insomnia,
Irritability,
Muscle weakness,
Weight loss,
Absence of menstruation,
Anxiety or nervousness,
Higher body temperature,
High blood pressure (i.e. fast heart rate),
Puffy eyes (i.e. abnormal protrusion of eyes), and
Increased BMR (Basal Metabolic Rate), etc.
Treatment :
Surgical removal of part or all of the thyroid gland (thyroidectomy),
Use of radioactive iodine to selectively destroy thyroid tissue, and
Use of antithyroid drugs to block synthesis of thyroid hormones.
Hyposecretion of thyroid hormone (Hypothyroidism) :
It is caused by deficiency of thyroid hormones or removal of thyroid gland (Thyroidectomy).
Cretinism :
In infants, hyposecretion (insufficient secretion or deficiency) of TH (or hypothyroidism) leads to Cretinism. The cretinism is also known as Congenital hypothyroidism. This condition causes severe mental retardation and stunted bone growth. At birth, the baby typically is normal because lipid-soluble maternal thyroid hormones crossed the placenta during pregnancy and allowed normal development.
Sign and symptoms of cretinism :
Poor feeding,
Excessive sleeping,
Weak cry,
Constipation, and
Prolonged jaundice (yellow skin) after birth, etc.
Treatment :
Congenital hypothyroidism is treated by giving thyroid hormone medication in a pill form called levothyroxine. Many children will require treatment for life.
Myxoedema :
In adulthood, hyposecretion (insufficient secretion or deficiency) of TH (or hypothyroidism) leads to Myxoedema. Myxedema, which occurs about five times more often in females than in males.
Sign and symptoms of myxoedema :
Weakness or lethargy,
Weight gain (i.e. obesity),
Anxiety or nervousness,
Depressed mood,
Low body temperature (feels cold),
Constipation,
Lacks of alertness,
Lacks of intelligence,
Stunted sexual development,
Goitre (i.e. enlarged thyroid gland),
Confusion or non-responsiveness,
Difficulty in breathing,
Low blood pressure (i.e low heart rate), and
Edema (i.e. swelling) of the body, especially the face, tongue, and lower legs, etc. Due to accumulation of interstitial fluid. And look puffy.
Treatment :
Myxedema is treated by giving thyroid hormone.
Simple goitre :
It is iodine deficiency goitre, iodine is required for synthesis of thyroid hormone and if there is deficiency of iodine in the diet, it causes enlargement of thyroid gland leading to simple goitre. This disease is common in hilly areas.
Sign and symptoms of simple goitre :
The size of the thyroid gland is increased but total output of thyroxine is decreased.
Treatment :
Addition of iodine to table salt to prevent this disease.
Disorders related to parathyroid gland :
Hypersecretion of parathormone (Hyperparathyroidism) :
Osteoporosis :
Hypersecretion (excess secretion) of parathormone (or hyperparathyroidism) leads to Osteoporosis. Hypersecretion of parathormone is responsible for more absorption of calcium from bones (i.e. demineralization of bones) resulting in softening, bending, brittle and fracture of bone. It is common in women, who have reached menopause,
Hyposecretion of parathormone (Hypoparathyroidism) :
Parathyroid tetany :
Hyposecretion (insufficient secretion or deficiency) of parathormone (or hypoparathyroidism) leads to parathyroid tetany. The parathyroid tetany is also known as Hypocalcemic tetany. It is a very rare disease. It causes neurons and muscle fibres to depolarize and produce action potentials spontaneously.
Sign and symptoms of parathyroid tetany :
This can lead to low levels of calcium in the blood, often causing cramping and twitching of muscles or tetany (involuntary or skeletal muscle contraction), and several other symptoms.
Treatment :
The primary treatment of hypoparathyroidism is calcium and vitamin-D supplementation.
Disorders related to adrenal gland :
Hypersecretion of adrenal hormones :
Cushing's syndrome :
Hypersecretion (excess secretion) of cortisol by the adrenal cortex leads to Cushing's syndrome. Cushing's syndrome is also known as Hypercortisolism. Causes include a tumour of the adrenal gland that secretes cortisol. A tumour elsewhere that secretes adrenocorticotropic hormone (ACTH), which in turn stimulates excessive secretion of cortisol.

Sign and symptoms cushing's syndrome :
Excess sweating,
Fatigue,
Headache,
Excessive hairiness,
Hyperpigmentation (i.e. darkening of the skin),
Flushing of face
Polyphagia (i.e. excessive hunger),
Insomnia,
Irritability,
Muscle weakness,
Weight gain or obesity (Pot belly),
Buffalo hump,
Osteoporosis,
Anxiety or nervousness,
Higher body temperature,
High blood pressure (i.e. fast heart rate),
Infertility, and
Abdominal stretch marks, etc.
Treatment :
Reducing steroid use,
Surgery,
Radiation, and
Medication, etc.
Pheochromocytoma (PCC) :
These are benign tumours of chromaffin cells of the adrenal medulla. These cause hypersecretion of epinephrine and norepinephrine.
Sign and symptoms PCC :
There is a prolonged version of the fight-or-flight response.
Excess sweating,
Fatigue,
Headache,
Dehydration,
Flushing of face,
Loss of appetite,
Insomnia,
Irritability,
Muscle weakness,
Weight loss,
Confusion or non-responsiveness,
Tremor,
Dizziness,
Anxiety or nervousness,
Shortness of breath,
High blood pressure (i.e. fast heart rate),
Hyperglycemia (i.e. high blood glucose),
Increased BMR (Basal Metabolic Rate)
Decreased gastrointestinal motility, etc.
Treatment :
Surgery to remove the tumour is usually required.
Hyposecretion of adrenal hormones :
Addison's disease :
Hyposecretion (insufficient secretion or deficiency) of glucocorticoids and aldosterone by the adrenal cortex leads to Addison's disease. The addison's disease is also known as Hypocortisolism. Addison's disease is the first discovered endocrine disorder. It is an autoimmune disorder in which in which antibodies cause; Adrenal cortex destruction and Block binding of ACTH to its receptors
Sign and symptoms of addison's disease :
Excess sweating,
Fatigue,
Headache,
Dehydration,
Hyperpigmentation (i.e. darkening of the skin),
Vomiting
Loss of appetite,
Insomnie,
Irritability,
Muscle weakness,
Weight loss,
Water-electrolyte imbalance,
Nausea,
Diarrhoea,
Dizziness,
Anxiety or nervousness.
Polyuria (i.e. excess urination),
Low blood pressure (i.e. slow heart rate),
Hypoglycemia (i.e. low blood glucose),
Absence of menstruation, and
Infertility, etc.
Treatment :
The primary treatment of hypocortisolism is hormone supplementation.
Disorders related to pancreatic islets :
Diabetes mellitus (DM) :
The most common endocrine disorder is diabetes mellitus caused by an inability to produce or use insulin. It is a disorder of blood glucose homeostasis. Diabetes mellitus is simply known as Diabetes. There are two major types of the DM;
Type-1 diabetes :
It is also known as insulin dependent diabetes mellitus (IDDM) or juvenile-onset diabetes. It usually arises in childhood. It is caused due to failure of insulin to facilitate the movement of glucose into cells. Reduced sensitivity to insulin is called insulin resistance.
Type-2 diabetes :
It is also known as non-insulin dependent diabetes mellitus (NIDDM) or adult-onset diabetes. It usually occurs after age 35 and becomes more common with increasing age. It is caused due to our regular diet.
Sign and symptoms of DM :
Polyuria,
Polydipsia, and
Polyphagia etc.
Treatment :
Diet,
Exercise,
Medication, and
Insulin therapy, etc.
Join the conversation